Introduction
Annually, non-communicable diseases (NCDs) are responsible for 41 million deaths which represents 74% of all deceases around the world. The four main types of non-communicable diseases are cardiovascular diseases, diabetes, chronic respiratory diseases, and cancer. Overweight/obesity, hypertension, hyperglycemia, and hyperlipidemia are metabolic risk factors that boost the risk of NCDs (1).
Abdominal obesity is defined as the excess of deposits of fat in the abdominal region, it represents an adverse form of obesity and an indicator of accumulation of triacylglycerols in the muscles and liver, which is why it is associated with cardiovascular disease, hypertension, diabetes, cancer, and kidney diseases (2).
Scientific literature establishes that abdominal obesity is a better predictor of cardiovascular disease than obesity measured by body mass index because of its direct relation with visceral fat (3). The most conventional method for assessing abdominal obesity is measuring the waist circumference and analyzing it according to sex-specific cutoffs (4).
The World Health Organization specifies that hypertension (≥140/90 mm Hg) is the leading cause of premature death in the world (5). Globally, around 1 in 4 adults have high blood pressure and only 50% of them know their condition. Additionally, the quantity of adults with hypertension raised from 594 million in 1975 to 1.13 billion in 2015 (6). An unhealthy diet, physical inactivity, excess alcohol consumption, and smoking are risk factors for developing hypertension (6). In Panama, 21.7% of the adult population had abdominal obesity in 2019, according to cut-offs points stablished by de International Diabetes Federation (≥90 cm (men) / ≥80 cm (women) (7). The Panamanian Ministry of Health reports that 36% of the population has hypertension (8). No studies were found that register data on abdominal obesity and hypertension in Panamanian college students.
Scientific literature has established an association between abdominal obesity and hypertension, high blood cholesterol, and hyperglycemia in the adult population (2,4,6,7). Evidence also links abdominal obesity with high blood pressure in college students from India (9). Despite this scientific evidence, there is not enough information on this topic for college students in Panama.
Therefore, this study aims to determine the association between abdominal obesity and hypertension, high blood cholesterol, and diabetes mellitus history in Panamanian college students. This information is crucial for designing strategies to promote healthy habits in this population by knowing their current levels of abdominal obesity and metabolic risk factor antecedents.
Materials and methods
This was an analytical cross-sectional study conducted on 434 college students from a private university in Panama between June and December 2022. The participants were selected through convenience sampling and included 306 women and 128 men out of 525 students who were invited to participate. Participants belonged to the faculties of Humanities, Health Sciences, Law and Social-Economic Sciences. They were enrolled in the second and third four-month academic period of 2022 and were of legal age. Only those who voluntarily agreed to participate by signing the informed consent were included in this study. Pregnant students and postgraduate students were excluded from participating.
The participants were informed about the research objective and procedures before providing verbal consent and signing the informed consent during the assessment session. After reviewing the required documentation and meeting the eligibility criteria, five professionals, including three physical therapists and two professionals in physical culture, recreation, and sports, applied the basic questionnaire of the STEPS World Health Organization Instrument (10). They also measured the waist circumference using Seca 201 measuring tape in the facilities of the Metropolitan University of Education, Science, and Technology, Panama (UMECIT).
Abdominal obesity was the dependent variable established as a waist circumference of ≥80 cm in women and ≥90 cm in men according to the International Diabetes Federation cut-off points for the Latin American population (11). Waist circumference was measured at the approximate midpoint between the lower margin of the last tangible rib and the top of the iliac crest by Seca 201 measuring tape. This measurement was realized at the end of a normal expiration, with the arms relaxed and over light clothing in a separate room (10).
High arterial pressure, diabetes mellitus, and high blood cholesterol history were the independent variables. The information on these variables was obtained through the basic questionnaire of the STEPS World Health Organization Instrument with the following questions:
¿Have you ever been told by a doctor or other health worker that you have raised blood pressure or hypertension?
¿Have you ever been told by a doctor or other health worker that you have raised blood sugar or diabetes?
¿Have you ever been told by a doctor or other health worker that you have raised blood cholesterol? (10).
Other variables such as sex, age, socioeconomic level, and current academic four-month period were also analyzed in this study. The research was conducted according to the Declaration of Helsinki and the Panamanian Ministry of Health (RESEGIS code 2489). The Bioethics Committee of the Metropolitan University of Education, Science and Technology, Panama (UMECIT) approved this research (CBI UMECIT 2022-06-16). Participants confirmed their participation in this study by signing the informed consent, which communicated the objective, the procedures to be carried out, voluntary participation, and the confidentiality of the data. Participants were identified by codes in the database to ensure their anonymity.
Data Analysis
This study analyzed descriptive characteristics of participants, describing categorical variables using frequencies and percentages and in the case of quantitative variables, depending on the distribution of the data, established by the Shapiro-Wilk test, variables that presented a normal distribution were described with the mean and standard deviation and in those that did not present a normal distribution, the median and the interquartile range were reported.
To determine a statistically significant difference according to sex, Fisher’s exact, Chi2, Student’s T, and Mann-Whitney's U tests were used. Bivariate analyses were performed between abdominal obesity and each of the independent variables, and those that presented values of p <0.20 entered the multivariate models.
Logistic regression models were used, using the dependent variable, such as dichotomous (abdominal obesity/No abdominal obesity) to establish the factors associated with the outcome of interest in this study. The data taken from the information collected through the described procedures were entered into an Excel database, which was exported to the Stata version 12.1 / IC statistical program to generate the results.
Results
Most of the participants correspond to the female sex (70,5%), they report a medium socioeconomic level (85,71%), and they were studying the first part of their professional career (69,82%). The mean age of participants was 21.55 (SD: 4.77) (Table 1).
Table 1. General characteristics of the study population stratified by sex
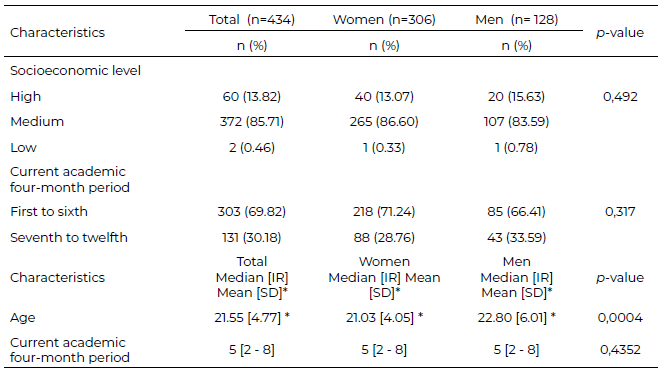
SD: Standard Deviation; IR: Interquartile Range
A little more than a third of the analyzed population registered abdominal obesity (36,41%). The antecedent with the highest report was hypertension (14,29%), followed by hiperlipidemia (13,82%) and hyperglycemia (9,22%). No statistical difference was found by sex (Table 2).
Table 2. Abdominal obesity and hypertension, hyperglycemia, and hyperlipidemia history stratified by sex in Panamanian college students.
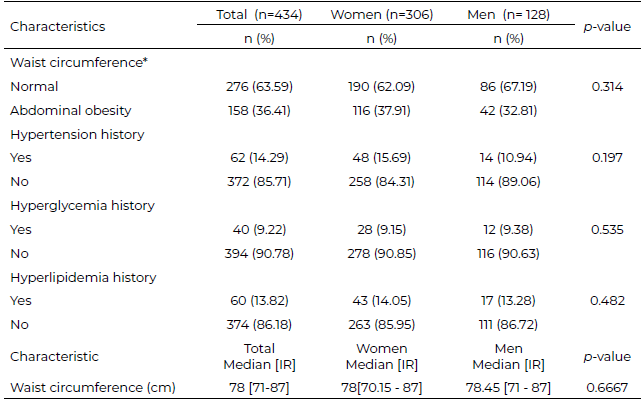
* According to International Diabetes Federation criteria, IR: Interquartile Range
After adjusting by sex, age, socioeconomic level, and academic four-month period, hypertension history was associated with abdominal obesity (OR:2.06, CI 95%: 1.183 – 3.597, p= 0.011) (Table 3).
Table 3. Association between abdominal obesity and hypertension, hyperglycemia, and hyperlipidemia history in Panamanian college students.
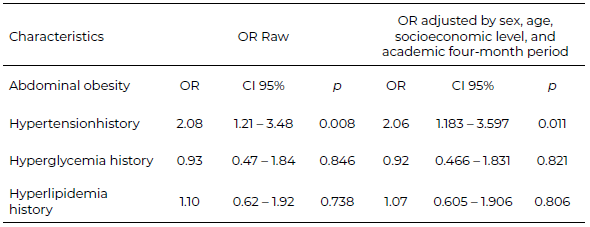
CI: Confidence Interval
Discussion
The study provides valuable insights into the prevalence of abdominal obesity and metabolic risk factors in Panamanian college students. The finding of an association between abdominal obesity and hypertension history is particularly noteworthy, as it can help design effective strategies to promote healthy habits in this population. The study also highlights the alarming rate of abdominal obesity among the participants and the potential risk of comorbidities associated with it.
Regarding abdominal obesity, 36.41% of participants had this risk factor. This result is higher than the one registered for the Panamanian adult population (21.07%) (7) and college students from Ecuador (25%) (12), and lower than college students from Bangladesh (39%) (13) Mexico (40%) (14) and Cuba (54.2%) (15).
The fact that almost 4 out of 10 participants in this study had abdominal obesity is alarming because, in Panamá, this condition represents a significant risk factor for developing and increasing comorbidity of diabetes, hypertension, and reduction in High-Density Lipoprotein Cholesterol (HDL) (7).
A possible explanation for the result of abdominal obesity in this study is that in Panama, in the last three decades, significant nutritional and lifestyle changes due to social and economic factors have contributed to increased sedentary behavior and diminished physical activity levels. In the specific case of the Panamanian diet, frying foods and high- sugar foods and beverages are common habits in this population, and daily consumption of food or beverages with elevated concentrations of sugar was associated with obesity (7).
In this study, the antecedent with the highest report was hypertension (14.29%), followed by hyperlipidemia (13.82%) and hyperglycemia (9.22%). This result is similar to the one registered in a research study that included 265 Panamanian college students that concluded that 12.45%, 11.11%, and 8.75% of the participants reported a history of high arterial pressure, high blood cholesterol, and diabetes mellitus, respectively (16). The result evidenced in this study is alarming considering the mean age of participants and is consistent with a systematic review that described metabolic risk factors in the Latin American College population (17).
The main finding of this study is the association between abdominal obesity and hypertension history which is by scientific evidence that has established this association in adult population (2,4,6,7) and in college students (9). Several factors explain why obesity is linked to hypertension history. Adipose tissue releases many bioactive mediators that have an influence not only on body weight homeostasis but also on alterations in lipids, coagulation, and blood pressure (18). Additionally, the expansion of body volume, the higher cardiac output, the declined systemic vascular resistance, the heightened activities of rennin-angiotensin-aldosterone, the elevated level of leptin, the increased free fatty acids, the excessive secretion of endothelin-1, and the disruption of natriuretic peptide activities along with the increased activation of the sympathetic nervous system are some of the factors that cause hypertension in obese people (19).
One of the limitations of this study is that there are different cutoff points definitions to determine central or abdominal obesity given by the WHO, the International Diabetes Federation, and the Adult Treatment panel III Guidelines, furthermore, cutoff point definitions also vary depending on sex, the use of different cutoff points could hamper comparisons among different studies (7). One of the strengths of this study is the use of international cutoff points to determine the abdominal obesity specifically in Latin American population (11).
This study recommends implementing strategies to promote healthy living habits to reduce future cardiovascular risk in the Panamanian university population. However, the study has some limitations, including a convenience sample and cross-sectional design, which only establishes an association between the variables and not causality.
In conclusion, A little more than a third of the analyzed population registered abdominal obesity. The antecedent with the highest report was hypertension. After adjusting by sex, age, socioeconomic level, and academic four-month period, students with hypertension history were more likely to have abdominal obesity.
Acknowledgments
This study was funded by the Metropolitan University of Education, Science and Technology of Panama, UMECIT.
Conflict of interest
The authors declare there is no conflict of interest.
Referencia
- World Health Organization. Non-communicable diseases. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases
- Dhawan D, Sharma S. Abdominal Obesity, Adipokines and Non-communicable Diseases. J Steroid Biochem Mol Biol. 2020; 203:105737. https://doi.org/10.1016/j.jsbmb.2020.105737
- Mohammadi H, Ohm J, Discacciati A, Sundstrom J, Hambraeus K, Jernberg T, Svensson P. Abdominal obesity and the risk of recurrent atherosclerotic cardiovascular disease after myocardial infarction. Eur J Prev Cardiol. 2020; 27(18):1944-1952. https://doi.org/10.1177/2047487319898019
- Kesztyüs D, Erhardt J, Schönsteiner D, Kesztyüs T. Therapeutic Treatment for Abdominal Obesity in Adults. DtschArztebl Int. 2018; 115(29-30):487-493. https://doi.org/10.3238/arztebl.2018.0487
- World Health Organization. Hypertension. Available from: https://www.who.int/news-room/fact-sheets/detail/hypertension
- Campbell NRC, Schutte AE, Varghese CV, Ordunez P, Zhang XH, Khan T, et al. São Paulo call to action for the prevention and control of high blood pressure: 2020. J Clin Hypertens (Greenwich). 2019; 21(12):1744-1752. doi: 10.1111/jch.13741. https://doi.org/10.1111%2Fjch.13741
- Montenegro Mendoza R, Velásquez IM, Fontes F, Quintana H. Prevalence of central obesity according to different definitions in normal weight adults of two cross-sectional studies in Panama. Lancet Reg Health Am. 2022 Mar 1; 10:100215. doi: 10.1016/j.lana.2022.100215.
- Ministerio de Salud de Panamá. Manejo de la hipertensión. Available from: https://www.minsa.gob.pa/sites/default/files/general/hipertension.pdf
- Jena S.K. Correlation of abdominal obesity indices with blood pressure in young adults: A cross-sectional study. Adv Hum Biol. 2018;8:46–48. https://doi.org/10.4103/AIHB.AIHB_50_17
- World Health Organization: WHO STEPS Surveillance Manual: the WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance. Geneva, Switzerland: World Health Organization, 2006. Available from: https://iris.who.int/bitstream/handle/10665/43376/9241593830_eng.pdf?sequence=1&isAllowed=y
- Zimmet P, K. Alberti G y Serrano Ríos M. Una nueva definición mundial del síndrome metabólico propuesta por la Federación Internacional de Diabetes: fundamento y resultados. Rev Esp Cardiol 2005; 58: 1371- https://doi.org/10.1016/S0300-8932(05)74065-3
- Alcívar JE, Campos NA, Plua WE, Peña M, Anderson HE. Riesgo cardiovascular antropométrico de estudiantes universitarios. Rev. cuba. cardiol. cir. cardiovasc. 2020;26(1):1–9. https://revcardiologia.sld.cu/index.php/revcardiologia/article/view/921
- Kamrul-Hasan AB, Chanda PK, Aalpona FZ, Ahsan A, Fatima M, Mahboob RN, Islam MA, Debnath CR. Frequency of Dysglycemia and Obesity among Undergraduate Students of a Medical College of Bangladesh. Mymensingh Med J. 2020; 29(3):539-544. https://pubmed.ncbi.nlm.nih.gov/32844791/
- Bueno C, Brito H, Delgado J, Dávila G, Petatan S, Pérez E, Rojas N. Predictores de riesgo antropométricos y bioquímicos para enfermedades no transmisibles en estudiantes de enfermería. Dilemas contemporáneos: educación, política y valores. 2020; 8(spe5), 00014. https://doi.org/10.46377/dilemas.v8i.2491
- Miguel-Betancourt M, Vázquez-González LA, Marchan- Bruzón M, Cue-López C, Curbelo-Videra W, Mason- Mayford A. Riesgo cardiovascular en estudiantes de medicina del municipio Puerto Padre de Las Tunas. Univ Méd Pinareña. 2020;16(3):1- 7. https://www.redalyc.org/journal/6382/638266621007/638266621007.pdf
- Rangel LG, Murillo AL, Pulido G. Asociación entre el sobrepeso y la obesidad con el colesterol, la presión arterial y la diabetes en estudiantes universitarios panameños. Rev Cubana Invest Bioméd. 2021;40(3):1-10. http://scielo.sld.cu/scielo.php?pid=S0864-03002021 000400009&script=sci_arttext&tlng=en
- Badillo RA, Rangel LG, Martínez R, Espinoza R. Prevalencia de factores de riesgo metabólico en estudiantes universitarios latinoamericanos: una revisión sistemática. Rev Salud Pública 2021;23(3): Epub Sep 03, 2021 https://doi.org/10.15446/rsap.v23n3.86164
- Van Gaal L., Mertens I. De Block C. Mechanisms linking obesity with cardiovascular disease. Nature. 2006; 444:875–880 (2006). https://doi. org/10.1038/nature05487
- Darsini D, Hamidah H, Notobroto HB, Cahyono EA. Health risks associated with high waist circumference: A systematic review. Journal of public health research. 2020;9(2). https://doi.org/10.4081/jphr.2020.1811
